




BACKGROUND
Niger is one of the poorest performing states in routine immunization (RI) in Nigeria. Only 39 percent of eligible children in Niger have received the Pentavalent 3 vaccine, translating to over 150,000 unimmunized children in 2020[1]. The high-cost of traditional training programs, continuous retirement of skilled healthcare workers, and limited health worker availability remain a challenge to human resource optimization for efficient and improved health service delivery. With 68 percent of local government areas (LGAs) classified as hard-to-reach, pulling healthcare workers out of their facilities to attend training sessions also contributes to the irregular provision of primary health care (PHC) services in the state. To address this issue, in 2017, the Clinton Health Access Initiative (CHAI) began implementing peer-led learning (PLL) as a low-cost approach to build health worker capacity at the convenience of their health facility. However, in 2021, a CHAI-led analysis of supportive supervision data on RI and observations from supervisors during field visits revealed suboptimal performance of peer-led learning which undermined the positive gains in immunization achieved through continuous learning approaches.
CHAI APPROACH TO OPTIMIZING THE CONDUCT OF PLL SESSIONS
To support the Niger State Primary Health Care Development Agency (NSPHCDA) to improve the implementation of peer-led learning in the state, the CHAI Niger team conducted an assessment to understand the root causes of suboptimal performance and provide solutions. The study found a need for:
- Improvements in peer-led learning implementation.
- Accountability for peer-led learning.
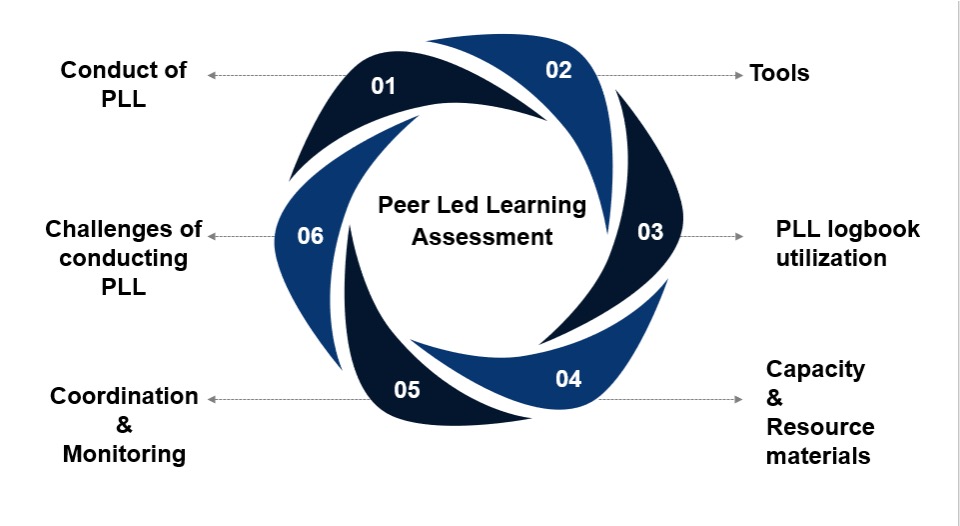
As highlighted in Figure 1, the peer-led learning assessment covered six key thematic areas.
Together with the NSPHCDA, CHAI conducted a quantitative assessment in September 2021, using a survey questionnaire. The team sampled 10 percent of health facilities (104) in the state from 13 LGAs targeting health workers. A minimum of four LGAs were randomly selected from each of the three senatorial zones, with eight health facilities selected per LGA.
ASSESSMENT FINDINGS
Key findings showed:
- 88.5 percent of healthcare workers reported suboptimal tracking and poor coordination as major reasons for low performance of peer-led learning across all the health facilities in the state.
- 66 percent reported non-use of PLL logbooks. Rough notebooks were used most for documentation as recorded in meeting minutes.
- About 63 percent reported they had not been trained on PLL. Half of the RI-related resource materials in storage were mostly used by health facilities that conduct PLL, thereby limiting PLL scope to RI only.
- Limited feedback on RI performance hindered health worker motivation, resulting in a lack of seriousness during peer-led learning sessions.
- 51 percent of sampled respondents provided reports on their PLL sessions; 59 percent indicated that there was no PLL schedule at their facilities. Hence, even when conducted, PPL sessions were non-routine and unstructured.
MILESTONES ACHIEVED
Through CHAI’s support, the state achieved specific milestones to improve PLL implementation, including:
- Developing and operationalizing state-specific and user-friendly PLL standard operating procedures (SOPs).
- Engaging, sensitizing, and motivating LGA Expanded Program on Immunization (EPI) managers on the strategic importance of continuous implementation, coordination, and monitoring of PLL in health facilities.
- Increased the proportion of health facilities conducting PLL from 48 percent in August 2021 to 53 percent in December 2021.
- Inclusion of PLL in the state annual operation plan for 2022.
LESSONS LEARNED FROM IMPLEMENTING PLL
There were several key takeaways from program implementation, including:
- The need for LGA/district teams to leverage monthly review meetings to monitor performance and provide feedback on PPL sessions for continuous improvement of healthcare workers.
- PLL should be integrated with e-learning platforms where they exist (i.e., Immunization Academy).
- PLL should be incorporated in health system recovery and improvement strategies as countries plan post- COVID-19.
RECOMMENDATIONS AND IMPLICATIONS FOR SCALE-UP
- Development of state-specific and user-friendly PLL SOPs remain pertinent.
- All health facilities should develop schedules for regular PLL sessions and share them with their respective LGA teams for proper monitoring and feedback.
- LGA teams should assign supervisors for all health facilities to provide regular updates on the progress of PLL during weekly or bi-weekly LGA meetings.
- Focal persons should be appointed in the state and LGAs to lead PLL sessions and train and mentor facility health workers.
- The state should develop a strong accountability framework in line with the civil service rule for good and poor performance.
This intervention was funded by the Bill and Melinda Gates Foundation. We also acknowledge the successful collaboration with the Niger State Primary Health Care Development Agency.
Authors: Mustapha Lawan, Senior Analyst, Vaccines Program; Rogers Kanee, Analyst, Vaccines; Daniel Jiya, Program Manager State Emergency Routine Immunization Coordination Centre, Niger State Primary Health Care Development Agency
Contributing Authors: Akachi Mbogu, Manager, Management System and Capacity, Global Vaccines; Destiny Olisadera Chukwu, Senior Associate, Vaccines Program; Dr. Shola Dele-Olowu, Deputy Director, Vaccines Program; Dr. Wiwa Owens, EVP Global Resources for Health, West and Central Africa Regional Director and Country Director Nigeria
[1] MICS-NICS 2021 Preliminary Estimates of Vaccination Coverage and Timeliness among Children Aged 12-23 Months, UNICEF

