




BACKGROUND
Limited health worker capacity and ineffective learning environments hinder optimal service delivery across primary healthcare (PHC) facilities in Kano State, Nigeria. Conventional training approaches that are often classroom-based, didactic, costly, and infrequent lead to service disruptions at points of delivery when they do occur. To create an optimal learning environment, supportive of effectively upskilling health workers, the Clinton Health Access Initiative (CHAI) introduced peer-led learning (PLL) in 2016—a low-cost, non-disruptive capacity-building approach to close health worker knowledge and skills gaps. In 2020, Immunization Academy (IA) was integrated into PLL as an additional learning platform for routine immunization (RI).
CHALLENGE
Peer-led learning was not without limitations which undermined uptake and sustainability in the state. Lack of monitoring mechanisms and visibility into PLL sessions by local government (LGA) and state agencies was the biggest challenge, affecting sustainability and ownership of the program by the government at all levels. Without this visibility, managers were unable to provide the necessary feedback essential for continuity and success.
INTERVENTION
To address the issue, CHAI developed an electronic Short Message Service (SMS), or text message, reporting platform in April 2021 to complement the paper-based logbooks used for tracking progress of PPL sessions. The SMS reporting platform enabled the state to have real-time data on the performance of peer-led learning sessions, including the number of sessions conducted, the number of participants involved, materials used, and topics discussed, directly from the facilities. The reporting platform leveraged existing structures in the state such as the Referral Network Service (RNS)[1] and Kano Connect closed-user group [2] to ensure sustainability and feasibility. At US$0.01, there is little cost burden to facilities to send SMS-based reports via the Kano Connect platform to LGAs.
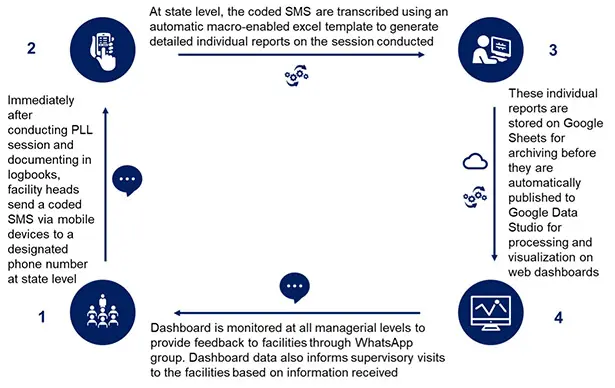
Figure 1: Flow chart of SMS reporting for PLL
Use of the platform was not challenging as health workers were already experienced with sending reports via the routine immunization (RI) SMS platform [3] and the state RNS. LGAs also easily accepted the platform as it allowed them to give real-time feedback; if reports were sent in the wrong format, were incomplete, or showed no records of sessions, LGAs could quickly follow up. WhatsApp groups were created to enable feedback between the health workers and their supervisors. These groups also provided an unintended platform for peer-to peer-learning where health workers could ask each other questions, share pictures, and provide encouragement.
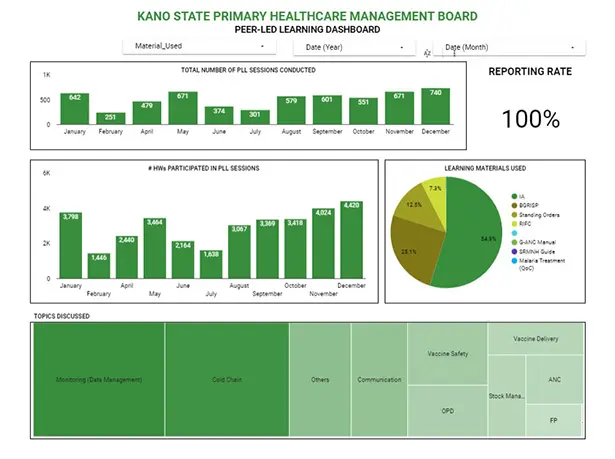
Figure 2: PLL Reporting Dashboard
CHAI trained a state focal person to manage the reporting platform, troubleshoot issues, and present monthly reports to the PHC working groups to encourage government ownership and sustainability. The availability of this data and visibility into facility-level capacity building improved the government’s interest and acceptance of the approach, especially since it provided simple, yet practical means for performance management and continuous quality improvement. In addition, the reporting platform allowed managers to track and monitor the use of IA by health workers which was difficult prior to the intervention. It also provided visibility into the number of health workers participating in each session, enabling easy quantification of health workers trained. In addition to immunization, other PHC programs such as antenatal care (ANC), sexual reproductive and maternal health, malaria, and family planning were also integrated into the platform, making it available to all health workers in a facility, irrespective of the services they provide.
IMPACT
Between April 2021 and January 2022, at least 5,000 health workers participated in over 6,000 PPL sessions on the platform; the reporting rate averaged 100 percent for participating facilities. The autonomy given to health facilities to plan, conduct, and select discussion topics during the sessions encouraged ownership as evidenced by increased uptake across facilities. It also empowered facilities to align their selected topics to their context. For example, during a period of extremely hot weather in the state in 2021, more than 70 percent of the sessions discussed cold chain management as facilities likely recognized that the weather conditions threatened the potency of vaccines. Using mobile phones for PPL sessions and reporting indirectly saved the government US$44,340 [4], which was then used to directly train or orient at least 4,400 health workers. The integration of other programs and inclusion of all health workers enables knowledge transfer among health workers from different programs. For example, ANC service providers shared that they gained better insight, particularly into how vaccines are arranged in the refrigerator, and RI providers leveraged the platform as an opportunity to refresh their skills and knowledge in child and outpatient care.
CONCLUSION
Technology provides unlimited opportunities to optimize processes, especially in settings riddled with challenges such as funding and resource constraints, bureaucracies, and paper-based tools. Digitization enabled real-time monitoring of PLL and made available data for informed decisions, feedback, and action. Opportunities exist to scale up this approach across the country to strengthen capacity building for overall improvement in quality of care.
Contributing authors: Hussaina Daradara, Assistant Program Officer, Vaccines Program; Balkisu Abubakar, Senior Analyst, Vaccines Program; Junaidu Barde, Associate, Vaccines Program; Destiny Chukwu, Senior Associate Vaccines Program; Shola Dele-Olowu, Deputy Director, Vaccines Program; Akachi Mbogu, Manager Area Owner, Management Systems and Capacity; and Dr. Owens Wiwa, EVP Global Resources for Health, West and Central Africa and Country Director Nigeria
This work was implemented in collaboration with Kano State Primary Healthcare Management Board through funding from the Bill & Melinda Gates Foundation.
[1] The Referral Network System (RNS) is an electronic platform for referring clients from primary facilities to secondary facilities through SMS
[2] Kano Connect Closed User Group is a system of communication between health facilities and the state managers through a designated telecom numbers fully funded by the state government to improve communication and coordination in the system
[3] SMS gateway is a platform that accepts data sent from an electronic hand-held device (phone)
[4] Extrapolated for each individual health worker from the average total cost for supportive supervision/spot-check per facility

