




Effective interventions to identify and reach underserved villages with immunization services
BACKGROUND
Beginning in November 2020, CHAI Uganda’s vaccines team set out to help the government address challenges with routine immunization service delivery and improve equity across 14 districts representing around 11 percent of the country’s children under five—about 952,000[1] children. These districts were identified as among the poorest performing in the Expanded Program for Immunization (EPI) in the 2016 national coverage and equity assessment
A CHAI assessment in December 2018 found that in the 14 focus districts there was limited interaction between health facilities and the communities they serve. This led to a poor understanding of the needs and challenges faced by communities with lower uptake of vaccination services. For example, 51 percent of health facilities conducting immunizations did not consider community care-seeking behaviors when planning for vaccination campaigns. In addition, health facilities were unable to systematically identify underserved communities within their catchment to use their limited resources in an optimal way, leading to a significant number of children un or under-immunized.
APPROACH
To address this, CHAI trained health workers on how to identify underserved villages proactively and systematically within their catchment areas and potential barriers to vaccination in these communities. The team supported dialogue between health workers and the communities which then informed designed interventions to drive vaccine uptake along with other primary healthcare services.
The team has piloted an intervention that monitors geographic variations in care-seeking trends in high-volume health facilities, detecting villages with the highest number of unimmunized (zero-dose) children within their catchment areas. CHAI trained national supervisors to mentor healthcare workers to make better use of available data to increase the equitable delivery of services. The assessments are conducted through monthly reviews of health facility immunization registers (HMIS072), which are compared to the expected numbers of infants derived from population estimates in each community.
Once these underserved villages are identified, CHAI supports health facilities to hold meetings with community leaders and influencers to understand the barriers to immunization and develop targeted mitigation strategies. While varied in nature, interventions include empowering community leaders with the correct information to sensitize their communities, engaging vaccine-resistant subgroups, optimizing immunization outreach sessions, assuring immunization service availability at local health facilities, and working together to track children who fail to complete their full immunization schedule.
IMPACT
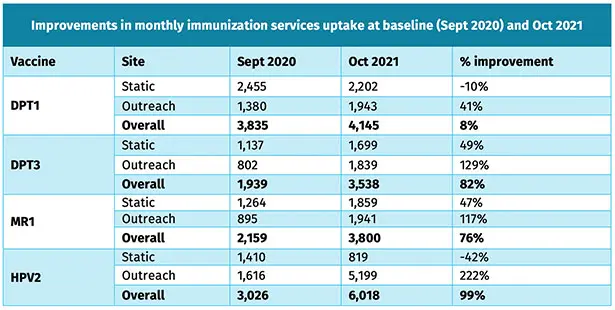
Table 1: Monthly number of children immunized at baseline (Sept 2020) and Oct 2021.
This work has led to increased vaccination rates in underserved villages. It has helped to improve the effectiveness of outreach sessions by targeting the underserved communities with high numbers of un- or under-vaccinated children. Overall, between September 2020 and October 2021, the number of children vaccinated for diphtheria, tetanus, and pertussis (DPT1 and DPT3), measles (MR1), and human papillomavirus (HPV2) increased by 82 percent, 76 percent, and 99 percent respectively, as indicated in Table 1. In addition, the number of children from underserved villages vaccinated against DPT3 and MR1 at static sites increased by almost 50 percent. Of significant note, the number of children vaccinated against HPV2 and MR1 greatly improved through optimizing the location, time, and frequency of outreach sessions, by 222 percent and 117 percent respectively.
LESSONS LEARNED
- This novel innovative and systematic approach to identifying underserved catchment villages has been well-received by healthcare workers (HCWs), as it uses smart analysis of available data in the child immunization register, rather than introducing new tools.
- Dialogue meetings between health facilities and communities are critical to identify and address unique root causes of low immunization uptake in underserved communities.
- The intervention helps health facilities optimally deploy their scarce human and financial resources to areas that are in dire need of services, as opposed to deploying broad interventions that are not well-targeted and require significant investments with limited results.
- Monitoring patient/caretaker health services can reliably inform and refine the planning processes, thereby tagging catchment villages to health facilities that are a true representation of where those people seek health services.
MOVING FORWARD
The 14 intervention districts were identified as among the worst-performing Expanded Program for Immunization (EPI) in the 2016 national coverage and equity assessment. After the implementation of CHAI-supported interventions, these districts are now outperforming average national immunization coverage across all vaccines as indicated in figure 1. This work, therefore, provides key insights for Uganda and other countries on impactful solutions to reach underserved and zero dose communities, as well as reducing missed opportunities for service uptake within health facilities. These results, albeit provisional, are critical in the context of ongoing COVID-19 disruptions to health services, which have negatively impacted infant vaccination coverage rates in many countries. The interventions can help inform service delivery models to support the recovery of immunization coverage to pre-COVID-19 levels and beyond.
CHAI will continue to support health facilities to institutionalize practices geared towards reducing missed opportunities for vaccination in early 2022. CHAI has worked actively with health facilities and district stakeholders to develop sustainability plans, which are being implemented, to ensure the long-term continuity of the activities while monitoring the performance and quality of the interventions. To enable national scale-up of these interventions, CHAI is working with Uganda’s Expanded Program for Immunization (UNEPI) and its stakeholders to ensure these tried and tested interventions are incorporated in the National Immunization Strategy 2022-2026 that is being finalized in the first quarter of 2022. For wider adoption in other geographies, CHAI is leveraging several international platforms for presentation as well as publication.

[1] 2020 UBOS Population projections
