




Senior Pauline was one of only three midwives on duty the night that Ankunda Teddy arrived at the Mubende Regional Referral Hospital in distress. The 28-year-old had been in labor for over 12 hours when she was referred to the hospital by a traditional birth attendant in Mubende district, Uganda.
Senior Pauline was eventually able to deliver the baby, but the child wasn’t breathing. She had been in this situation before.

A pediatrician from UPA and midwives working in Mubende RRH going through a simulation session on newborn resuscitation.
She had seen too many infants die of asphyxia and hypothermia because of a lack of training to handle the situation. In the past, necessary resuscitation equipment was kept in the neonatal intensive care unit (NICU) located at the other end of the hospital – too far away when every second counted.
But this time it was different.
“I had been trained and mentored on helping babies’ breath and a resuscitation corner had just been established within the maternity ward with all the equipment and drugs I needed,” said Senior Pauline.
She resuscitated the infant, wrapped her in a clean, warm blanket, and provided the antibiotics needed to save the baby’s life that night.
November is Prematurity Awareness Month. Globally in 2019, 2.4 million children died in the first month of life and Sub-Saharan Africa had the highest neonatal mortality rate in the world at 27 deaths per 1,000 live births, according to the World Health Organization.
Birth asphyxia, the failure to establish breathing at birth is one of the leading causes of neonatal mortality in Uganda contributing up to 27 percent of all neonatal deaths. Prematurity increases the risk of birth asphyxia by 11.97 times (Amina and Wahya, 2016). For infants born prematurely, which is defined as three weeks before their due date, the numbers are even more stark.
Helping Babies Breath is a high impact intervention used globally to reduce neonatal mortality due to birth asphyxia. In Uganda, CHAI has been working with the Ministry of Health and professional bodies to introduce the integrated intervention.
A case study in Mubende Regional Referral Hospital
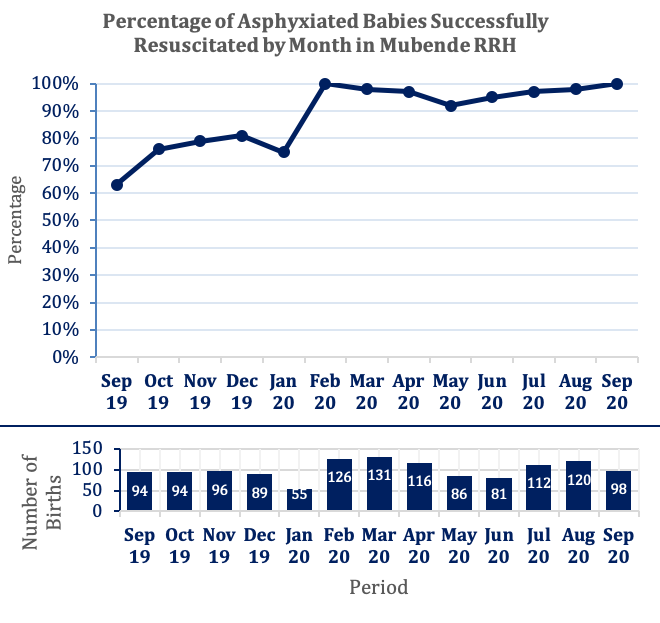
In June 2019, CHAI conducted a baseline assessment at the Mubende Regional Referral Hospital, the only hospital in Mubende District. The assessment showed that only 63 percent of asphyxiated babies born at the hospital were successfully resuscitated (against the WHO recommended standard of 95 percent).
At the time, care providers had inadequate newborn resuscitation knowledge and skills as well as inadequate availability of basic breathing aids for newborn resuscitation; such as a penguin sucker, a suction bulb to remove mucus clogging an infant’s nose and mouth, or a bag and mask to provide positive air pressure to open the neonatal airway.
Accessing the equipment that was available could be difficult, as it was not kept in the maternity ward. The assessment also found inconsistence or inappropriate use of the partograph – a composite graphical record of key data entered against time on a single sheet of paper – to monitor women in labor.
An integrated approach to clinical mentorship
Results from the baseline assessment were shared with the Mubende Regional Referral Hospital Board and frontline health workers from the maternity ward and NICU. With support from CHAI, a National Quality Improvement team was formed, with mentors from the Ministry of Health, the Association of Pediatricians (UPA), and the Association of Gynecologists and Obstetricians (AOGU).
The team trained midwives in the maternity ward on Helping Babies Breath techniques and provided ongoing mentoring. The maternity ward was re-organized to make space for the equipment needed to enable immediate resuscitation of babies born with asphyxia. The new resuscitation corner contained a bag and mask, a penguin sucker, tetracycline eye ointment for eye care, dry clean cloths to keep babies warm, a thermometer to monitor body temperature, a stethoscope, and vitamin K.
“Before CHAI, MoH, and AOGU conducted the mentorship program, many of the stillbirths were due to birth asphyxia. This time, I had been trained. I could quickly and confidently save the life of Teddy’s baby.”
– Senior Pauline, Midwife at the Mubende Regional Referral Hospital
One of the midwives on duty was responsible for the resuscitation corner, monitoring usage and replacing equipment. The daily work schedule was adjusted so that a more skilled health worker was always paired with a less experienced one. The team also incorporated simulation sessions into their routines. Midwives had to practice on a simulator to perfect their skills before they began to treat asphyxiated babies.
These changes produced dramatic results.
After the training and initial mentoring to improve providers’ knowledge and skills, the percentage of asphyxiated babies successfully resuscitated increased from 63 percent in September 2019 to 79 percent by November of that year.
After establishing a neonatal resuscitation corner in the maternity ward, this percentage rose to 100 percent by February 2020.
In the period since, the figures have consistently remained above 90 percent, with the most recent data for September 2020 showing that every single newborn with asphyxia was again successfully resuscitated. This means that an estimated 35 babies survived in one month alone, where previously they may have been lost.
The Way Forward
This mentorship model has been so successful because it uses data to develop the right solution for the situation, focuses on improving the everyday processes that health providers use to strengthen the entire system, and relies on a dedicated team to carry out the work.
The results at Mubende Regional Referral Hospital have been lifesaving. CHAI is now supporting the Ugandan Ministry of Health to review the national quality improvement framework and strategic plan to replicate this model in other districts.
With contributions from Ivan Kayondo and Rachael, Maternal, Newborn and Reproductive Health – Uganda.
