




Every year, billions of dollars allocated to health in low- and middle-income countries fail to reach the frontline—not because funds aren’t allocated, but because the systems moving money are broken. Traditional approaches rely on expensive implementation of financial systems over many years. Digital public infrastructure could be a key enabler to address this challenge. In a new report, CHAI and eGovernments Foundation describe how a different approach can change this and set out the practical steps to get there.
In the past year, the global health community has been consumed by a painful question: how do we do more with less? Foreign aid cuts and fiscal space constraints have forced difficult trade-offs. But alongside this challenge, another is equally critical: how do we ensure the limited funds available are spent and make it to the frontlines.
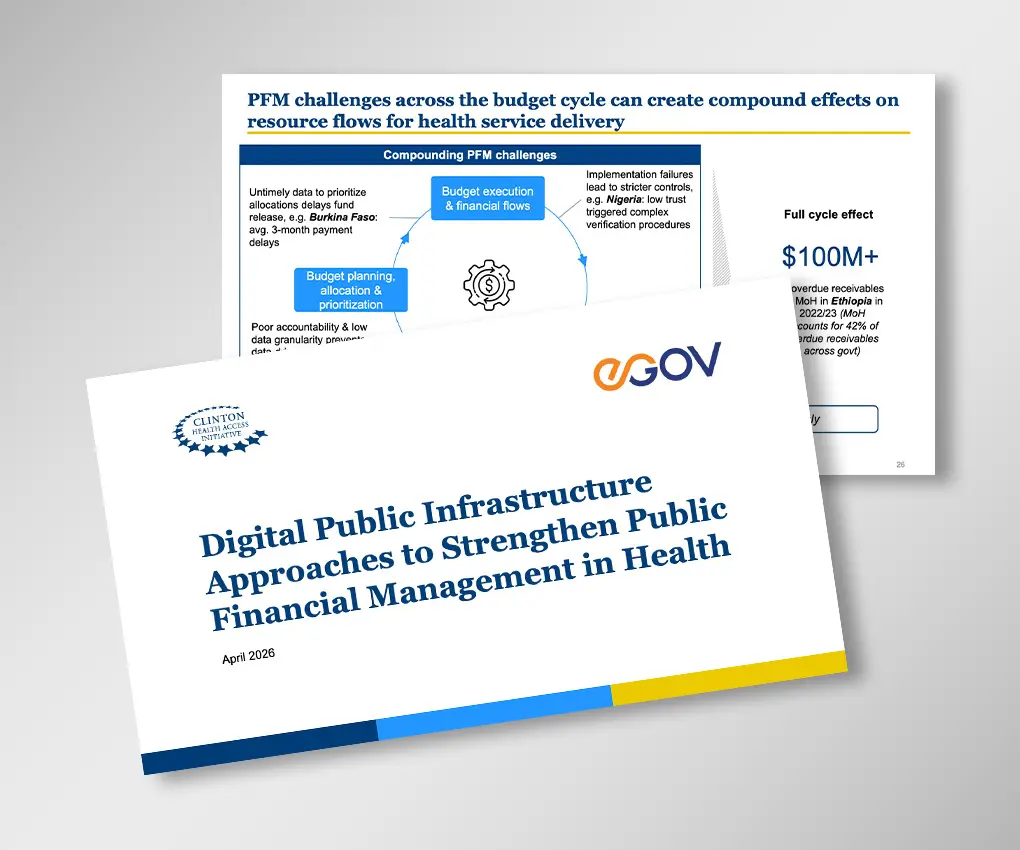
A community health worker in Burkina Faso went six months without pay. Not because funding ran out, but because fragmented identity records and manual verification meant the payment system could not confirm who she was or what services she had delivered. US$3.25 million in medication expired in a warehouse in Eswatini while nearby facilities went without. Not because procurement had failed, but because no system connected stock visibility at the center to the facilities that needed it. Similarly in Ethiopia, a major pooled donor fund often spends less than 50 percent of its budget. Not because the need isn’t there, but because limited procurement visibility and fragmented reporting systems mean money is delayed or poorly documented.
These are not outliers. A World Bank analysis of 64 low- and middle-income countries found that 15 percent of government health budgets go unspent. The situation is often worse for highly verticalized and earmarked donor budgets—where underspend is estimated to equal what low-income sub-Saharan African countries spend on primary healthcare. The money is often there, but the systems to move it are fragmented or dysfunctional.
As donors increasingly look to channel resources through country systems rather than around them, the quality of those systems and the accountability they can bring matter more than ever. But strengthening them doesn’t have to mean years-long technology assessments and overhauls. Digitizing transactions closer to the source and applying common data standards can increase visibility and accountability without replacing what already exists.
Why the traditional approaches to public financial management in health fall short
In the early 2000s, governments progressively turned toward Integrated Financial Management Information Systems and Enterprise Resource Planning platforms to unify data across sectors. The promise was compelling: real-time data for decisions makers across all sectors and all spending. But these tools were built for finance ministries, not health service delivery. They focus on central treasury operations rather than facility-level transactions. Data is aggregated before it enters the system, losing the granularity needed for real decisions.
This means governments lack the visibility needed to allocate and move money; and the consequences are felt most at the frontline. When logistics and finance systems use different facility codes and cannot exchange data, procurement is based on historical estimates rather than actual facility need. Medicines pile up centrally while facilities run out of stock. When completed work sits in paper reports awaiting manual verification, six months can pass before a health worker is paid.
How digital infrastructure can strengthen financial management in health
Decades of experience with these systems point to a simple truth: this is not just a systems problem, it is a standards problem. Each ministry, donor, or program maintains its own classifications, meaning systems cannot communicate and exchange information reliably.
The solution is not another standalone system. Think of it like roads and railways: shared digital infrastructure built once, that everything else can run on—rather than stakeholders building their own disconnected standards and tools from scratch. Applied to financial management, shared foundations act as a digital backbone connecting systems that already exist, rather than replacing them.
This approach is already delivering results.
In India, work completion data from the field was made quickly verifiable and attributable to the workers who performed it, creating a trusted information flow up the multiple levels to the state financial system (IFMIS). This reduced the wage payout timeline from 144 days to 12—a 92 percent reduction that didn’t replace the underlying financial infrastructure. In Nigeria, cross-checking government payroll against biometric data and bank verification numbers identified 23,846 ghost workers that could be removed from government payroll, enabling monthly savings of US$11.5 million. Across 23 countries, WHO-supported payments to polio campaign workers using existing mobile money infrastructure cut disbursement times from weeks or months to under 10 days. None of these required a multi-year system overhaul. They required shared standards and interoperability to leverage and connect systems that already existed.
Practical guidance for governments and funders
CHAI and eGovernments Foundation’s new report, Digital Public Infrastructure (DPI) Approaches to Strengthen Public Financial Management in Health, draws on consultations across 14 countries in Africa and Asia to offer practical guidance for governments, implementers, and funders: how to apply a DPI approach to financial management systems, which enabling conditions matter most, and how digital tools can be applied in low- and middle-income countries to make the most of limited resources without investing in major reforms.
We have also documented our scoping process for this work, which you can follow with the guidance here: Download Scoping Guidance
To note: This report is based on research funded by the Gates Foundation. The findings and conclusions contained within are those of the authors and do not necessarily reflect positions or policies of the Gates Foundation.
