Despite an observed increase in the cost of quality treatment for malaria in the private sector – where most people seek care – patients are still opting for the recommended treatments over cheaper, poorer-quality options.
Despite significant gains in reducing the burden of malaria since 2010, malaria remains one of the leading causes of death and infant mortality globally. Nigeria, Uganda, and Kenya are responsible for 76 million malaria cases, over one-third of total global cases. When seeking care for malaria, the private sector is often the first consult and primary source of care in these countries. However, regulatory oversight is often absent or not enforced so there is limited insight into the quality of care provided in this sector.
In 2006, the World Health Organization (WHO) introduced Artemisinin-based Combination Therapy (ACT) as the recommended first-line treatment regimen for malaria. However, due to the high cost of ACTs, many patients in the private sector were using ineffective and poor-quality monotherapies to treat malaria. To help improve the affordability and availability of ACTs in the private sector, the Affordable Medicines for Malaria (AmFM) program was introduced in several malaria-endemic countries including Nigeria and Uganda to subsidize donor-funded, quality-assured ACT brands (WHO-PQ-ACTs) for the private sector. These subsidies succeeded in reducing the retail price of WHO-PQ-ACTs by as much as 10-fold and helped increase availability from nine to 27 percent at baseline to 53-83 percent at endline in six countries. The co-payment mechanism (CPM) followed AMFm and continued to lower prices for WHO-PQ-ACTs, however the program was terminated in Kenya and Nigeria in 2018 and reduced in Uganda.
Since the end of AMFm/CPM, CHAI has closely monitored the commodity market, conducting cross-sectional retail audit assessments in Kenya (2019), Nigeria (2016, 2018, 2021) and Uganda (2014, 2018, 2020). Audits helped to track changes in availability, pricing, and market share of ACTs in the private sector since the removal of the payment schemes.
We summarize a few our key findings:
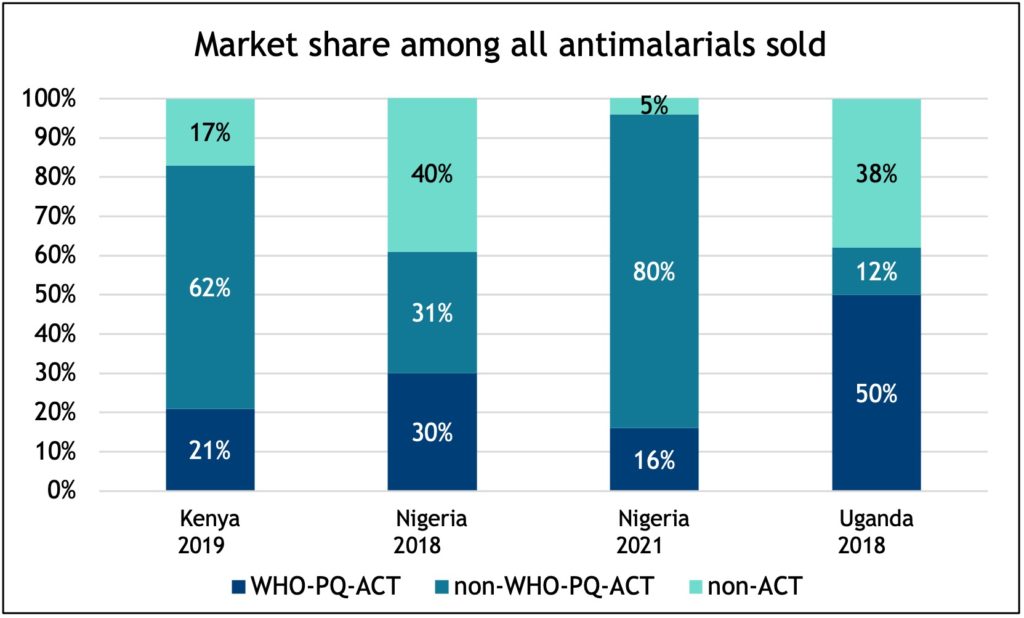
1. The AmFM and CPM programs were a success and a game changer for crowding out monotherapies and increasing the availability of WHO-PQ-ACTs in the market, hence improving access to appropriate malaria case management. For example, post-CPM, the market share of oral monotherapy significantly reduced in Nigeria from 30 percent in 2018 to less than five percent in 2021.
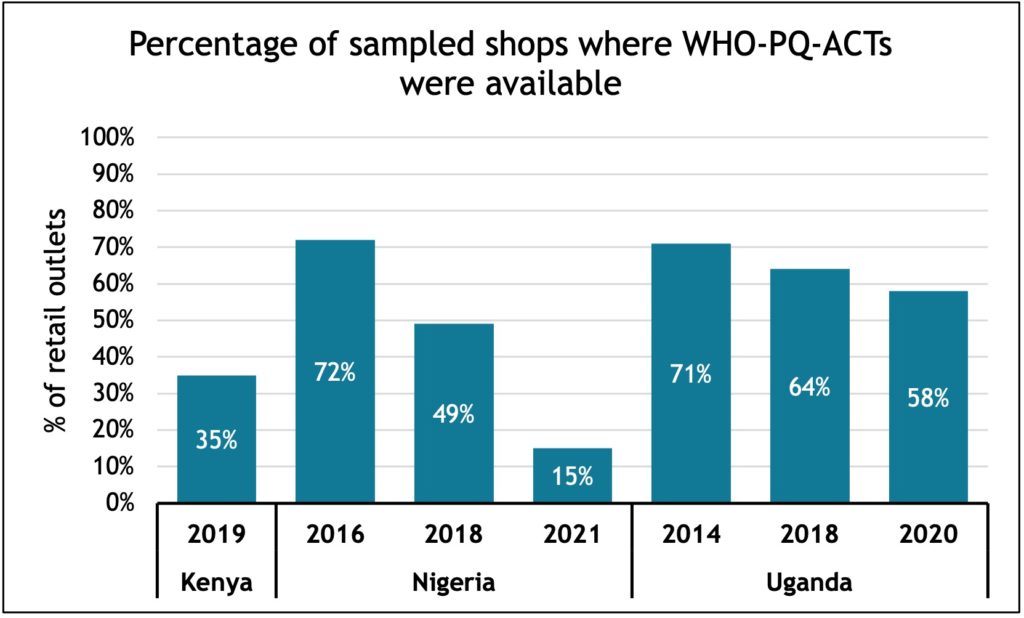
2. Decreasing availability of WHO-PQ-ACTs with time was observed across all three countries. This is possibly due to the high cost of these commodities compared to ACTs which are not prequalified by WHO (non-WHO-PQ-ACTs), cheaper and more available in the market.
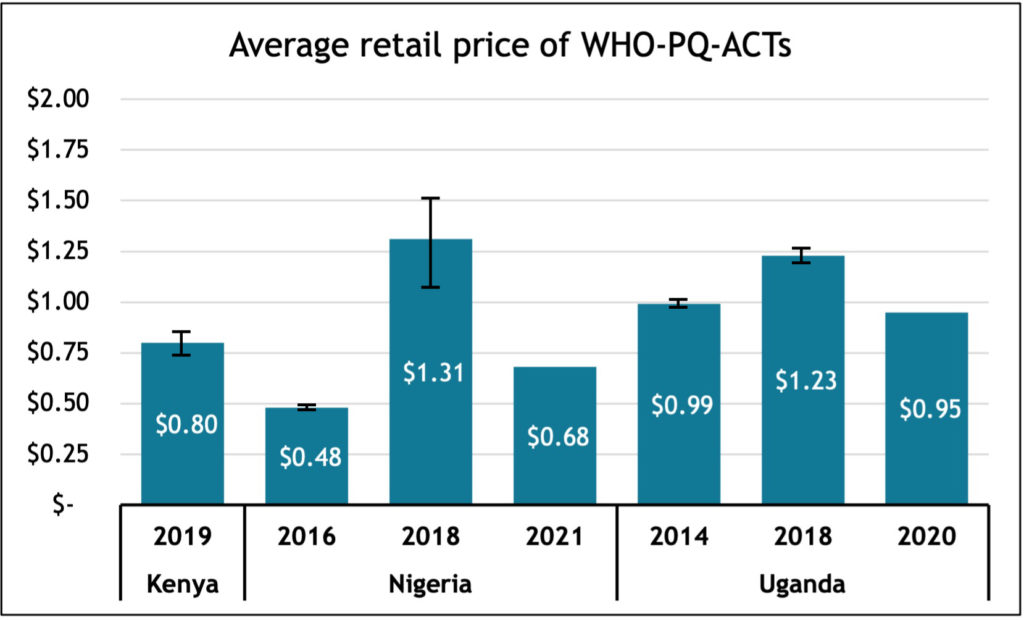
3. Decreasing affordability of WHO-PQ-ACTs: Pre-AmFM, pricing was one of the biggest constraints to accessing ACTs in the private sector. Over the years, the average retail prices of WHO-PQ-ACTs in the private sector has fluctuated over the years in Nigeria and Uganda, however with the reduction of subsidies in 2018 we are seeing prices increase.
Our results indicate that WHO-PQ-ACT availability and market share has declined while non-WHO-PQ-ACT availability and market share has increased. This trend coincided with the decrease in ACT subsidies through CPM. In Uganda, where the CPM is still in place, we see higher market share of WHO-PQ-ACTs and availability compared to Nigeria. Although such surveys provide useful information on the private sector market, they can be costly and conducted infrequently. Better routine data on ACT and RDT use will help us understand testing and treatment practices and enable national malaria programs to monitor and respond to barriers in the quality of services provided by the private sector.