




Background
Hypoxemia, characterized by low oxygen levels in the blood, contributes to over 800,000 preventable global deaths annually, particularly among children and neonates. Inadequate provider skills and oxygen supply management systems have hindered the timely diagnosis and treatment of hypoxemia, resulting in avoidable fatalities. This program, in partnership with the Ministry of Health and CHAI, aims to enhance healthcare provider skills and strengthen health systems for effective hypoxemia management in 31 healthcare facilities in 16 districts across Uganda.
Ensuring a competent and motivated healthcare workforce is essential for delivering high-quality healthcare services. Hypoxemia significantly increases the risk of mortality by 5.4 times, yet it often goes undiagnosed and untreated due to gaps in provider knowledge and skills. A baseline assessment of 31 health facilities revealed that 82 percent of healthcare workers lacked in-service pulse oximetry training, and 72 percent had not received oxygen administration training.
Theory of Change
Providing quality hypoxemia management services is critical for improving patient outcomes – oxygen therapy can reduce pediatric pneumonia mortality by up to 35 percent and hospital stays from seven to three days. Timely hypoxemia case detection is vital, and healthcare workers should be proficient in using pulse oximetry for screening. To bridge these knowledge and skills gaps, the Ministry of Health Uganda and CHAI implemented a health system strengthening program aimed at expanding access to hypoxemia diagnosis and treatment. The program focused on training healthcare workers, providing mentorships, and utilizing the quality improvement (QI) methodology to address systemic barriers to quality care.
Approach
Integrated onsite training, mentorships, and QI coaching were conducted to improve provider competence in hypoxemia management. National mentors were enlisted to establish a group of regional trainers proficient in hypoxemia management and QI methodologies.
Regional trainers were assigned to specific facilities for continuous onsite clinical mentorships and QI coaching. These trainers cascaded their knowledge to frontline healthcare workers, with a focus on pediatric wards, Neonatal Intensive Care Units, emergency departments, and outpatient departments. Health facility QI teams were established or revamped, with hypoxemia management and oxygen therapy becoming integral components of the team’s improvement objectives.
Frontline healthcare workers formed work improvement teams (WITs) and implemented rapid Plan-Do-Study-Act (PDSA) cycles to enhance hypoxemia diagnosis and treatment. Bi-monthly integrated onsite mentorships and QI coaching sessions were conducted to further develop provider skills and assist WITs in overcoming systemic barriers to quality hypoxemia management.
On a quarterly basis, WITs convened for peer-to-peer workshops, facilitating the sharing of innovative, scalable solutions aimed at improving access to hypoxemia diagnosis and treatment.
Impact/Results
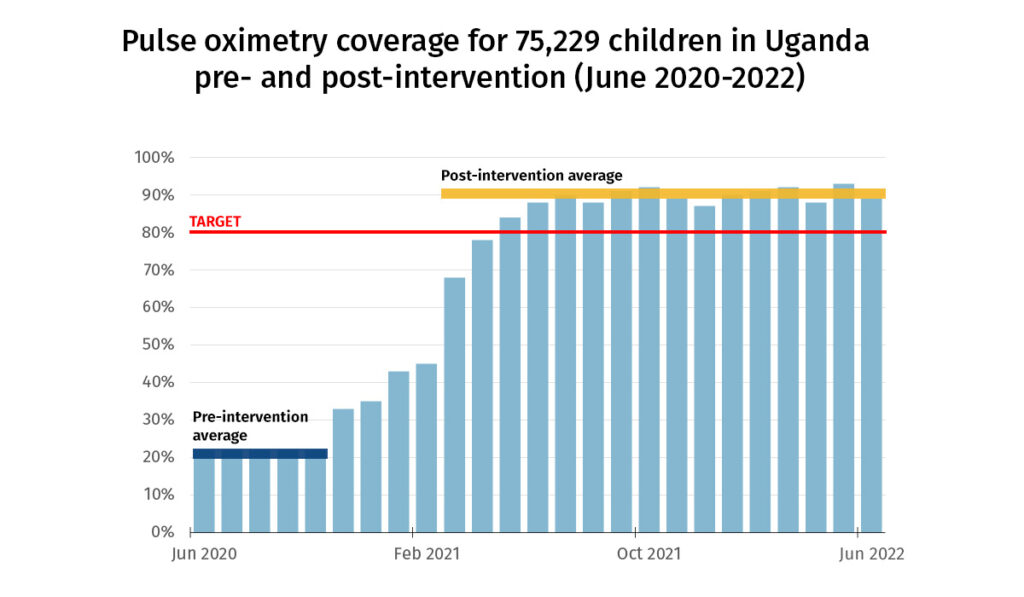
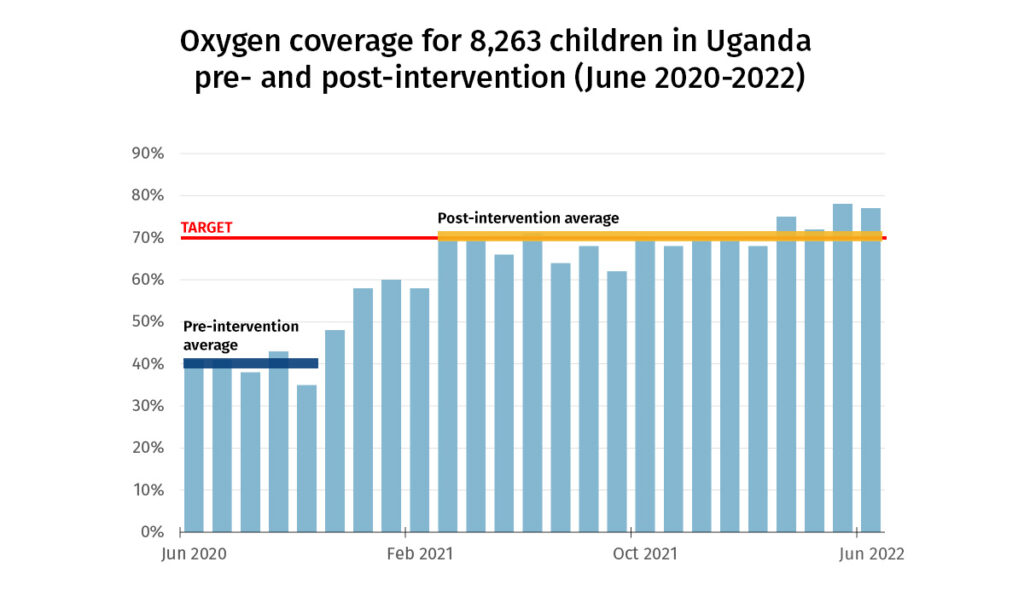
There was an increase in the use of pulse oximetry to diagnose hypoxemia and the use of oxygen to treat patients (0-15 years) diagnosed with hypoxemia, as shown in the chart below.
Facility Level High-Impact Tested Changes
- Peer-to-Peer Mentorships: One of the cornerstones of our program has been the establishment of peer-to-peer mentorships focused on hypoxemia management and the proper use of oxygen equipment. These mentorships have proven to be effective in enhancing the skills and knowledge of healthcare workers.
- Routine Hypoxemia Screening: At triage, we have introduced the adoption of routine hypoxemia screening using pulse oximetry. This has significantly improved our ability to identify patients with low blood oxygen saturation levels promptly.
- Rubber Stamp for Vital Observations: The introduction of a rubber stamp displaying vital observations, including blood oxygen saturation (SpO2), has served as a reminder for healthcare providers to record these essential parameters consistently.
- Color-Coded Cards: We have implemented the use of color-coded cards to expedite the identification of patients with a blood oxygen saturation level below 90 percent, ensuring timely intervention.
- Clinic Flow Adjustment: To facilitate efficient oxygen administration, we have adjusted the clinic flow at the Outpatient Department and pediatric ward, incorporating an emergency corner for oxygen administration.
Lessons Learned
- Establishing competent facility-based oxygen champions has been instrumental in the swift integration of hypoxemia management into program sites.
- Providing onsite training, mentorship, and QI support has enabled trainees to translate theoretical knowledge into practical skills seamlessly. This minimizes interruptions to service delivery and identifies and addresses health systems barriers effectively.
- Involving Assistant District Health Officers has ensured ownership of the program at district levels, which has facilitated timely follow-up on action plans, ensuring the continuity of the intervention.
- Collaboration with facility management has ensured prioritization of hypoxemia management and its incorporation into facility budgets, enhancing sustainability.
Next Steps
- Building upon the best practices and lessons learned in the Mubende and Jinja regions, CHAI will scale this intervention to other regions across the country. Our aim is to make hypoxemia management accessible to a wider population.
- CHAI is actively collaborating with the Ministry of Health (MOH) and learning institutions to incorporate hypoxemia management into the pre-service curriculum. By doing so, we hope to equip future healthcare workers to manage hypoxemia effectively.
- A Training of Trainers model continues to build the capacity of more healthcare workers in public and private health facilities.
Additional Information
- Plan-Do-Study-Act (PDSA)
- Hypoxemia prevalence and management among children and adults presenting to primary care facilities in Uganda: A prospective cohort study
- Management of hypoxemia

