




Background
More than ever before, the Ethiopian private health sector is playing a pivotal role in children’s healthcare. The health statistics system, DHIS2, shows that about 15 percent of children in Addis Ababa receive their vaccinations from private health facilities. In addition, a 2019 assessment of the Ethiopian private health sector revealed that approximately one-third of children received treatment for diarrhea at a private facility. While the private sector’s contribution to childhood vaccinations has increased, the quality of care remains poorly understood and under-documented.
In 2020, there were 34 private health facilities in Addis Ababa providing childhood immunization and maternal health services. But now there are 45. Even then, the facilities received little oversight and guidance from the government. There were no mechanisms to enforce quality immunization services, including vaccine storage and administration, cold chain management, reporting of coverage, and adverse events following immunization (AEFI). The linkage between the private and the public health sectors was and remains weak.
Approach
In 2020, the Clinton Health Access Initiative (CHAI), supported by Gavi, designed and implemented a project to support private health facilities in Addis Ababa to strengthen the quality of immunization services. CHAI worked closely with the Addis Ababa Regional Health Bureau (RHB) and sub-city health offices to provide technical assistance in the coordination, planning, and monitoring of routine immunization services in private health facilities. Working in close collaboration with the Ministry of Health (MOH), the project began with the revision of the national immunization implementation guide. The guide was updated to include the roles and responsibilities of private health facilities in delivering routine immunization services. CHAI conducted a baseline assessment of private facilities to evaluate critical elements for the delivery of quality immunization services. Based on the results and in consultation with the Addis Ababa RHB, we identified priority interventions to improve the quality of services and linkages to government health structures.
CHAI also performed continuous supportive supervision and trained staff to ensure the availability of essential resources and quality of care in the facilities. The training included in-depth reviews of the National Immunization In Practice guidelines, recording and reporting best practices, and vaccine supply management across 45 facilities. We also facilitated cross-sector learning, arranging for public healthcare workers to share their experiences in delivering quality immunization services with their counterparts in the private healthcare sector. As a step up from the cross-sector learning, we ensured the lessons learned, best practices, and implementation tools were shared broadly during review meetings.
In addition, CHAI helped establish a forum for private health facilities under the supervision of the Addis Ababa City Administration Health Bureau (AACHB) to improve routine immunization services. The forum brings together the AACHB, representatives from five private health facilities, MOH, Addis Ababa Food and Drug Administration (AA FDA), the private health facilities’ association, sub-cities representatives, and implementation partners (CHAI, WHO).
After a year and a half of implementation, CHAI conducted an end-line assessment to evaluate and document program successes. The lessons from this work in Addis Ababa have been used to scale up interventions to private health facilities in other urban centers in the country.
CHAI also conducted a cross-sectional quantitative study comparing baseline and end-line results across the 45 private health facilities. CHAI collected data through SurveyCTO and analyzed it using Z statistic to identify areas of improvement between the baseline and end-line results.
Results
At least 45 private health facilities in 11 sub-cities in Addis Ababa were visited for the end-line assessment, as depicted in Figure 1. The map shows the distribution and location of PHFs included in the end-line assessment activities.
Figure 1. PHFs that provide routine immunization services in Addis Ababa, July 2022
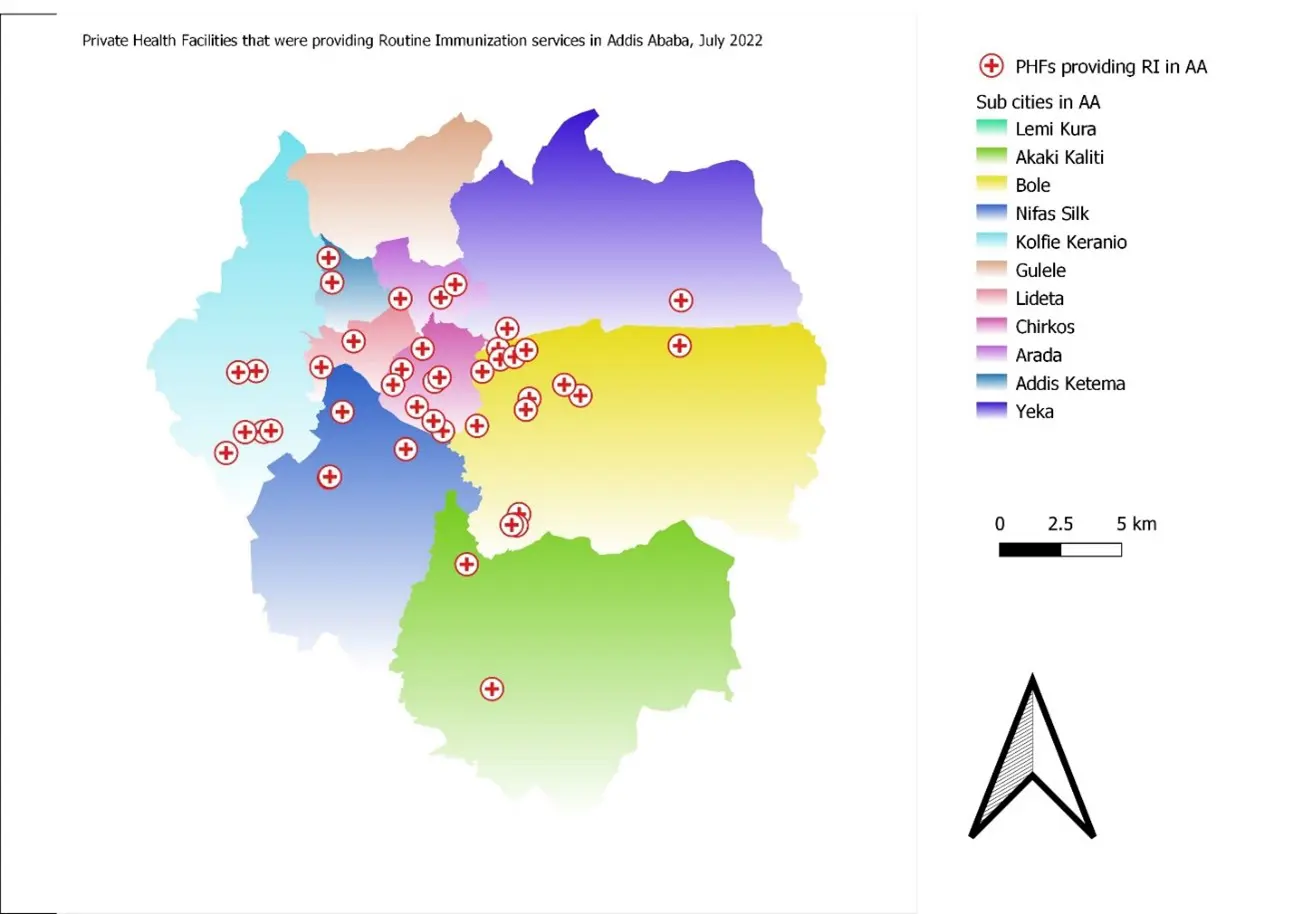
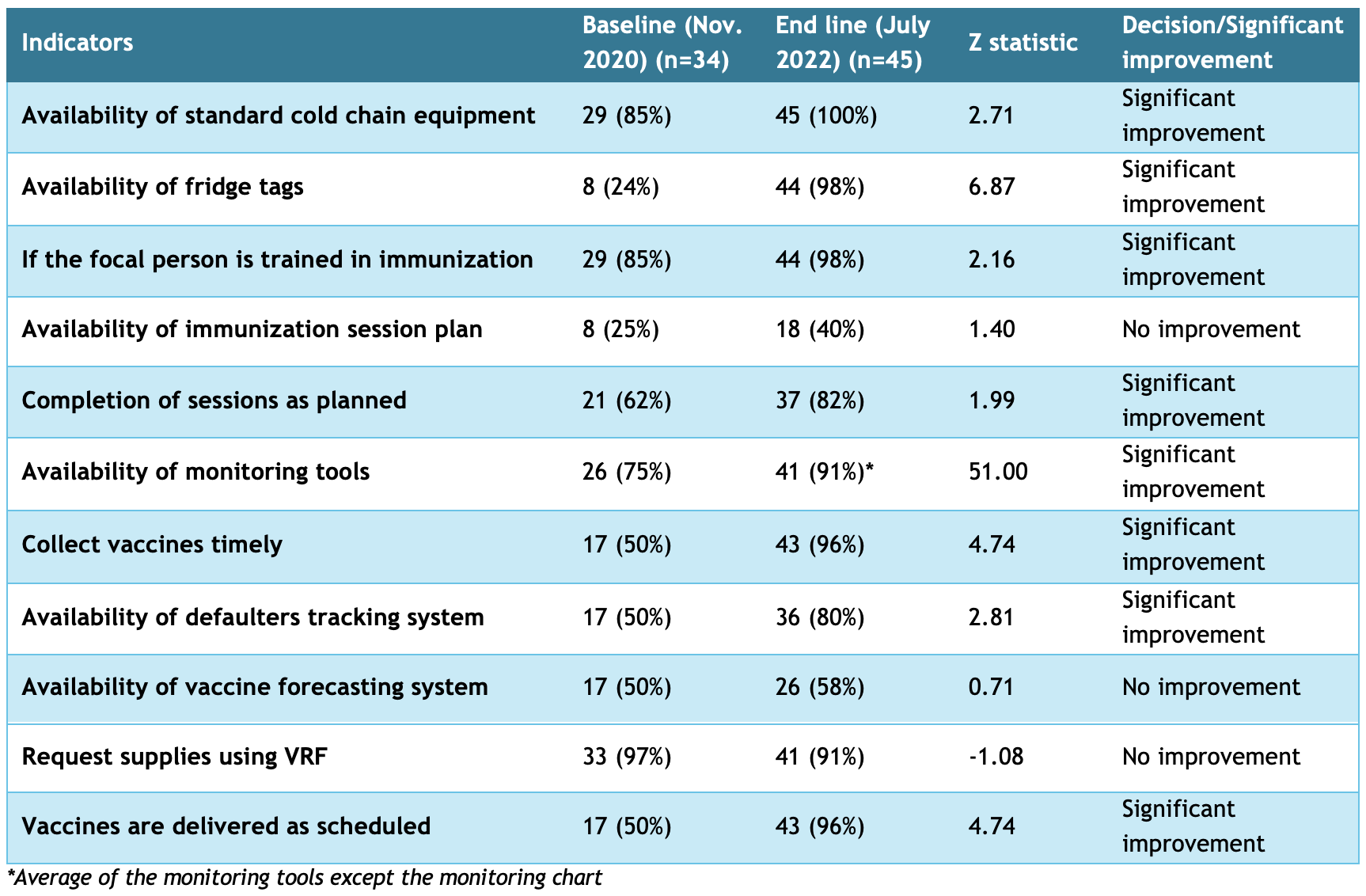
The number of private health facilities providing immunization services increased from 34 during the baseline assessment in November 2020 to 45 at the end of the project in July 2022. While 15 percent of private facilities did not have pre-qualified refrigerators at baseline, by end-line, all the 45 private health facilities had standard immunization refrigerators. Likewise, almost all (98 percent) facilities had fridge tags (either built-in or standalone) at the end line point compared to only 24 percent at baseline. The number of trained staff increased from 85 to 98 percent at end-line. The availability of standard routine immunization recording and monitoring tools also improved from 75 percent at baseline to 91 percent at end-line.
Only 40 percent of facilities at end line planned for routine immunization services, indicating room for improvement. However, this still represents a 25 percent increase from the baseline. Furthermore, 96 percent of facilities at the end line, compared to 50 percent at baseline, collected and delivered vaccines in a timely fashion. At least 80 percent of facilities at end line had a defaulter tracking system to identify children who may have missed their next vaccination dose compared to 50 percent at baseline.
In general, Table 1 shows that the quality and availability of immunization services being provided at private health facilities significantly improved, ensuring quality and access to immunization services. The Z test run over the baseline and end line proportions’ data showed that the difference (the improvement) is significant at a 95 percent confidence level for most variables except the availability of vaccine session plans, vaccine forecasting system, and requesting of vaccine supplies using the government VRF system.
Table 1. Comparison of selected indicators between baseline and end line, July 2022
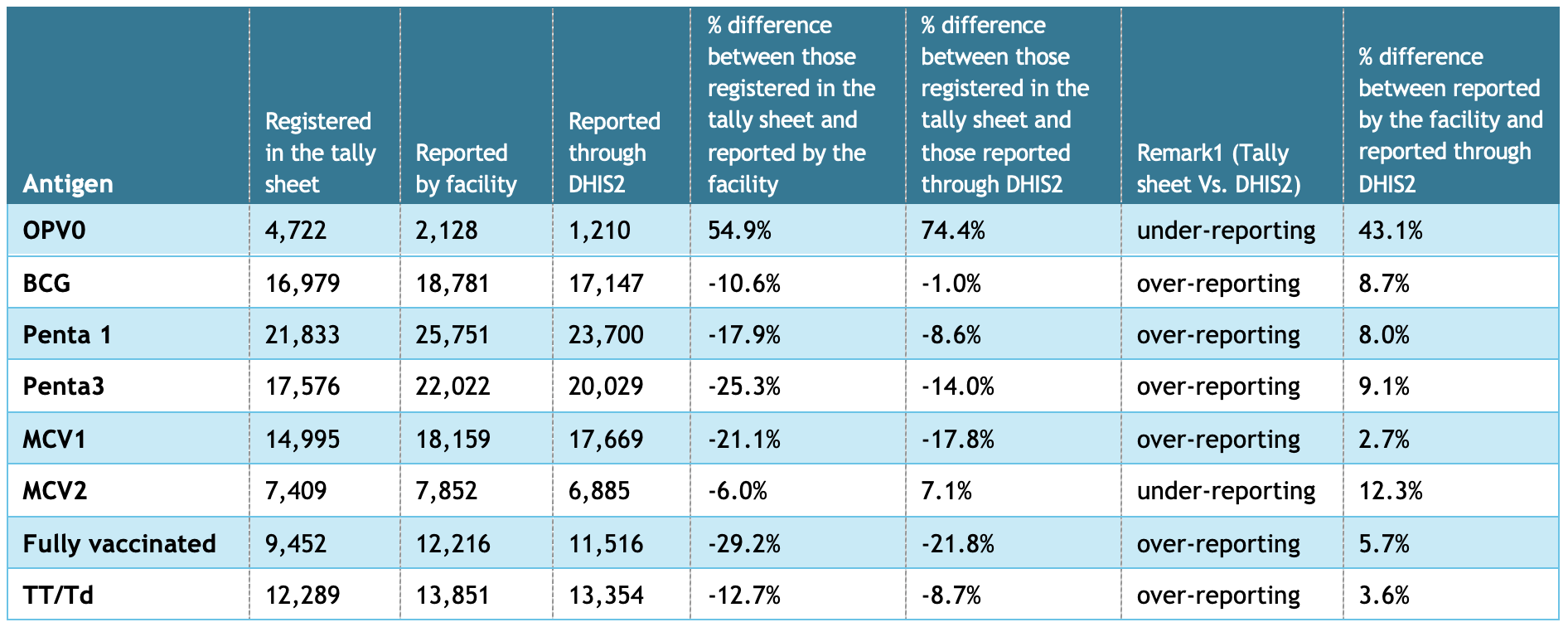
The linkages between private health facilities and government structures also improved significantly. By end line, 96 percent of private health facilities acknowledged support from the Regional Health Bureau. The support was primarily in the form of supportive supervision and the provision of immunization registers, tally sheets, reporting formats, stock recording books, and VRF. However, only 20 percent of private facilities respondents were aware of a formal written public-private partnership agreement (e.g., fully executed MOU) for the provision of immunization support services. Despite these improvements, challenges remain, particularly in data quality. The one-year aggregated vaccination data from private health facilities in Addis Ababa for 2014 EFY (2021/22) showed that there is a wide variation between the number of vaccinated children recounted from the tally sheets and those reported through DHIS-2 system in almost all antigens. Comparing these datasets, most antigens are found to be over-reported, while OPV0 and MCV2 are under-reported. The over-reporting could be due to human error or lack of oversight for data collection and accurate reporting, while the under-reporting could be due to the gap in reporting through DHIS2. Some of the PHFs have direct access to DHIS2 reporting, while others do not have it, and the sub-city/HCs report for them. (See Table 2). These findings are similar to the findings in Ghana[1].
Table 2. Data quality issues in PHFs in Addis Ababa, July 2022
Conclusion
The private sector contributes a significant share of health services in many countries, including Ethiopia. Public–private partnerships have gained significant global policy attention in recent times and have been implemented by a growing number of countries. Public–private partnerships are essential in moving towards universal health coverage to fill gaps in coverage and prevent governments from overstretching their capacity to deliver for all.[2]
In Ethiopia, the public-private partnership has led to significant improvements in the quality of immunization services delivery in the private sector. This has been achieved using pre-qualified cold chain equipment, training of healthcare workers, and improved use of government tools and systems. These findings are in line with those from other different studies in similar settings.
Lessons Learned to improve quality of immunization services in the private sector:
- Holding training sessions on routine immunization at least annually is important to address high staff turnover and maintain the quality of services.
- Supportive supervision of private health facilities is also critical as a capacity-building mechanism and to strengthen partnerships with government structures.
- Private health facilities should be encouraged/required to use WHO-prequalified refrigerators to maintain optimum temperature and ensure vaccine potency.
- Private health facilities welcome the opportunity to provide immunization services and to establish strong working relations with public health facilities for uninterrupted supplies and services.
[1] Sorengmen Amos Ziema and Livingstone Asem, Assessment of immunization data quality of routine reports in Ho municipality of Volta region, Ghana, BMC Health Services Research (2020) 20:1013 https://doi.org/10.1186/s12913-020-05865-4
[2] “Role and contribution of the private sector in moving towards universal health coverage” World Health Organization. Regional Office for the Eastern Mediterranean – p. ISBN: 978-92-9022-074-9
