




Why do people not seek care when they have symptoms suggestive of TB?
Tuberculosis (TB) killed 1.4 million people in 2019. India accounts for more than a quarter of the 10 million people who get sick with TB around the world each year. While there have been improvements in the quality of and access to TB treatment, significant gaps remain in care seeking, with 42 percent of Indians with TB not getting diagnosed on time.
Getting people to go to the doctor as soon as they have symptoms is a big part of the problem we need to solve. This requires a deeper understanding of what drives someone’s choices to seek care (or not) and their journey, a critical first step in developing a precision public health strategy.
To deploy such a strategy in a country with a high burden of TB, Clinton Health Access Initiative (CHAI) partnered with Surgo Foundation and the Greater Chennai Corporation (GCC). From 2018 to 2019 we investigated why people in the southern Indian city of Chennai did or did not seek prompt care for TB symptoms. Our motivation for identifying barriers to care was simple: to develop innovative, precise interventions to address them.
We started by conducting a first-of-its-kind, large-scale, prospective, community-level study, surveying over 85,000 households across Chennai, finding 1,700 participants with presumptive TB symptoms. We found that employed men (42-60 years old) who consume alcohol drink or smoke had the highest risk of getting TB yet sought care at the lowest rates. Among this group, the top reasons for not seeking care included low-risk perception and time constraints due to work and family obligations. We identified other segments, such as retired and unemployed men and employed women, and found each segment had different reasons for seeking care or not for TB.
Given this information, we are now able to segregate population groups based on their behavior, and we can contextually target them. Thus precision public health to ensure that we deliver the right solutions to the right people at the right time, using the best available data and technologies is warranted in our approaches to combat TB. In Chennai, we are now designing and implementing interventions to improve risk perception and provide more convenient TB services customized to each segment’s needs.
This work has shown us the need for TB programs to adopt this precision public health approach to address the different drivers of care-seeking across population segments. In the following sections, we detail the insights and implications of our care seeking study in Chennai, illustrate the value of a precision public health approach, and share the opportunities we see for its applications for TB programs across India and around the globe.
Study Findings: Employed men do not seek care because of low-risk perception and time constraints
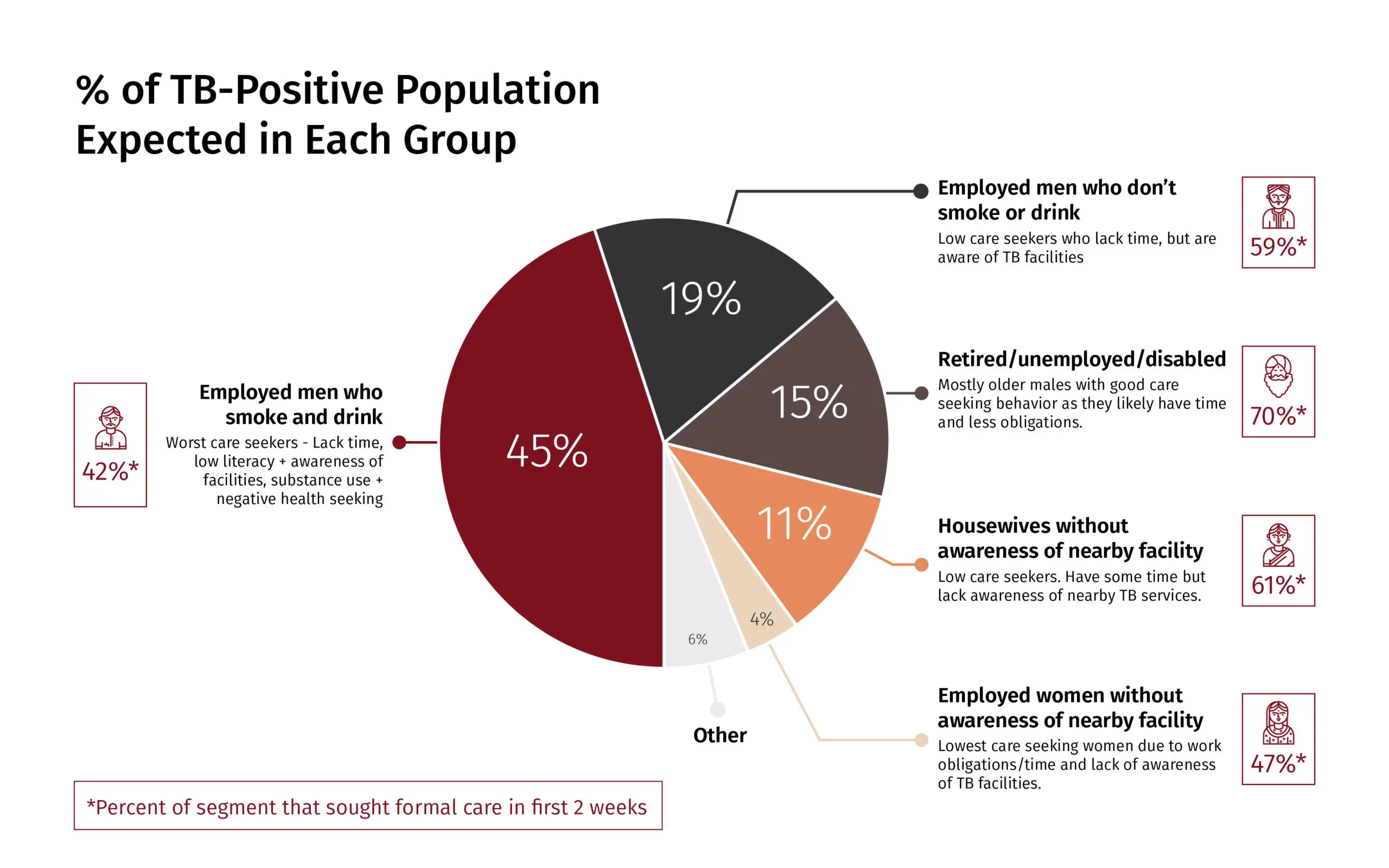
Percentage of TB-positive population expected in various cohorts of the Indian population.
To understand why presumptive TB patients do not seek care, we identified the predictors of care-seeking, mapped the care-seeking journey in real-time, and identified population segments with similar care-seeking behavior. Our findings suggested the need to target the segment of employed men for more focused TB screening, especially those who problem drink and smoke as they have the highest risk of becoming TB-positive while also being the least likely to seek care (only 42percent seek care vs. 70 percent for retired men).
While previous studies identified awareness of TB as a gap, our study found that low-risk perception, as well as a lack of time, were the most important predictors of low care-seeking. Notably, time constraints were a bigger barrier to care-seeking than financial constraints. This suggested the need to customize TB interventions to patients’ needs and making it more convenient to seek care. Beyond the initial doctors’ visit, provider-switching and low rates of provider- recommended testing led to further care-seeking delays. In addition to provider-training, another way to address this gap is to create clear expectations of the testing process and empower patients to ask for a test from their provider.
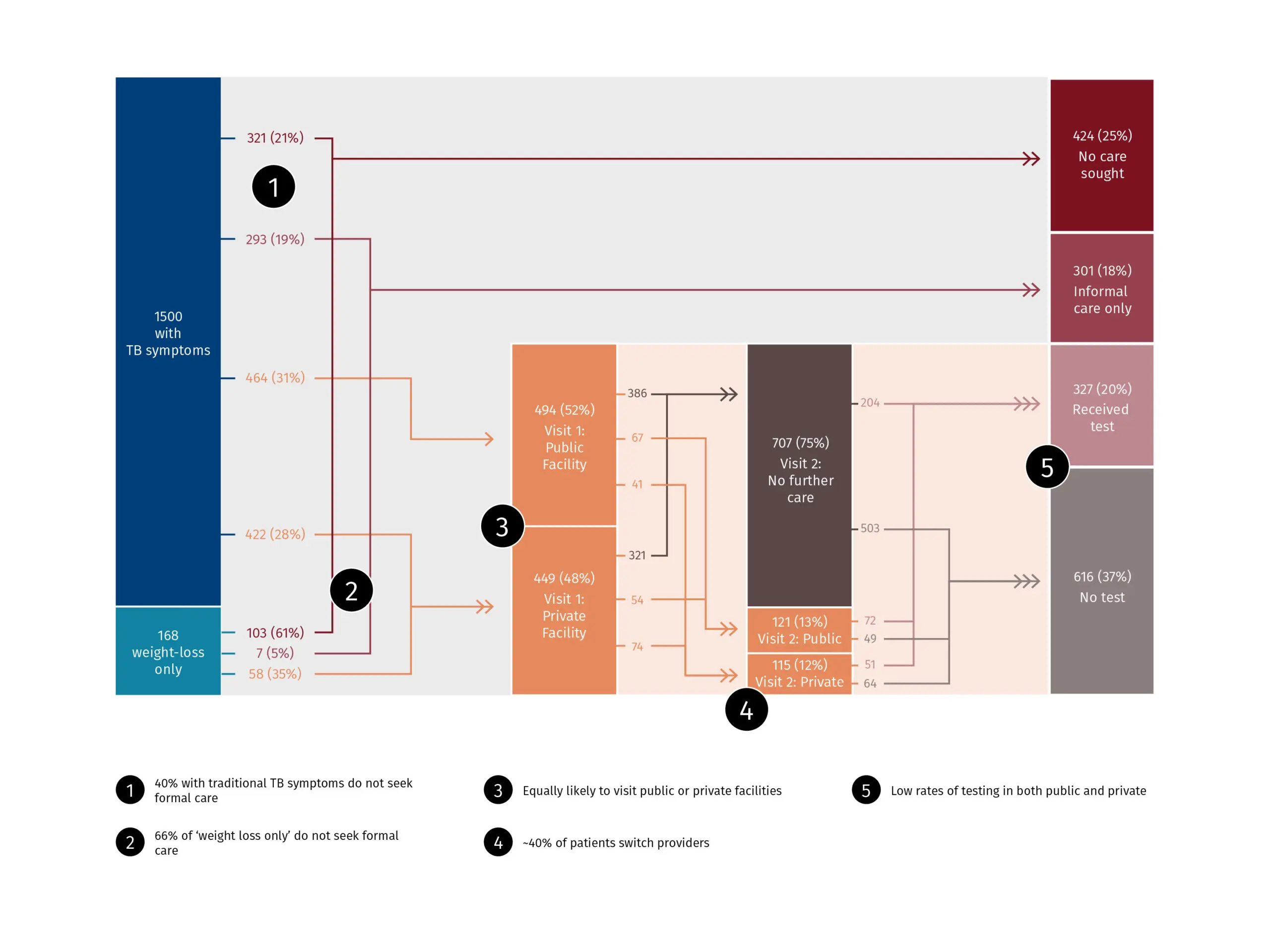
Community survey results show patients’ care-seeking journey.
Implications: We must bring the right TB interventions to the right people at the right time
Global TB programs should adopt a user-centric, precision public health approach that can increase care-seeking and close the TB gap. This means moving beyond a one-size-fits-all approach to target specific groups with specific interventions that address their identified barriers. This approach is based on asking three key questions that apply to nearly every public health program:
- Who to target? TB programs need to move from generalized screening to targeted screening of specific groups. More granular target groups can be identified by enhancing current geographic and demographic targeting with psychobehavioral segmentation to understand what is driving behavior for each segment. In Chennai, this means targeting subpopulations with high TB risk and low care-seeking behavior e.g. employed men who problem-drink or smoke to address the barriers of low-risk perception and lack of time.
- How and where to reach them? We need to reach people where they are. Depending on the context, this may include congregate settings such as communities, churches, and workplaces or targeting them through mobile phones. In Chennai, given the highly mobile nature of target groups, CHAI and Surgo are partnering with the government to pilot innovative digital channels and target new in-person settings to reach presumptive TB patients. Through these channels, we will explore targeted interventions such as customized messages to encourage care-seeking and tools to provide information on convenient TB services. This will include the ability to schedule appointments and/or receive reminders to go and seek care.
- With what services? In addition to routine services, we need to make it as easy and convenient as possible to seek care. Taking a customer-centric approach could include door-to-door services, weekend and after-hours services, and workplace screenings. It would require a shift from largely facility-centric models to more flexible, decentralized, community-based service. In the era of COVID-19 and social distancing, digital entry points and telehealth can play a bigger role in target group mobilization and service provision. While telehealth is already being used for TB treatment and adherence counseling, it can also be a low-cost, remote alternative to conduct TB symptom screening, triage, and testing referrals.
Next Steps: Implement, measure, scale, and replicate
We see great potential in applying a precision public health approach for TB. In Chennai, we are currently designing and implementing approaches to target specific groups (employed men) with customized interventions using novel channels to meet them where they are, including digital means. We are also testing models for delivering convenient, and flexible TB screening and testing services that are available for them when they do seek care.
This novel approach to address TB care seeking gaps will be one of the first systematic applications of comprehensive digital approaches to target men for TB care-seeking. We look forward to sharing the results once ready so they can be scaled up and replicated for other global public health programs and in other countries.
